Pathologic fracture is a broken bone with dislocation or without dislocation that occurs by minor trauma (for example as a result of a sitting transfer or of turning in bed) The causes of pathologic fracture include the area weakened by osteolytic metastases, diffuse osteoporosis or by the combination of both.
Pathologic osteolysis is the predominant symptom in multiple myeloma patients (occurs in 50% of patients). Nevertheless, the pathologic osteolysis may develop in all the other types of mclassant lymphoproliferative disorders and in many other cancerous diseases. The highest incidence rate of bone metastases is observed in patients with lung cancer, breast cancer and kidney cancer but may be associated with other mclassant diseases. Non-mclassant causes include bone cyst, osteomyelitis, osteoporosis, osteodystrophy, osteopoikilosis and Paget´s disease. Bone pain is the most frequent presenting clinical symptom of the patients with MM that have developed a lytic lesion (in 80% cases).
Impending Pathologic Fracture (Mirels´ scoring system)
The presence of a large lytic lesion is related to the risk of pathologic fracture. Lesions in long bones (and in other parts of skeleton) weaken both trabecular and cortical structure significantly increasing the likelihood of fracture. The load-bearing capabilities of bones are reduced and microfractures develop resulting in severe pain. The Mirel´s scoring system quantifies the risk of pathologic fracture due to cancer metastases to the bones. /see the table below/.
|
Points |
1 |
2 |
3 |
|
Site |
upper limb |
lower limb |
peritrochanter. |
|
Pain |
mild |
moderate |
severe |
|
Type of metastasis |
blastic |
mixed |
lytic |
|
Size (related to bone diameter) |
< 1/3 |
1/3-1/2 |
> 2/3 |
A high risk of pathologic fracture is predicted for patients with a mean average score exceeding 7 points.
The site, the size, the character of the lesion as well as the intensity of pain are important factors to assess the risk of fracture. The rate of fracture is only 5% when the lesion is 1/3-2/3 of the diameter of the bone. But the rate can increase up to 81% in case the lesion is greater than two thirds of the diameter of the bone. Lytic lesions are a result of a more advanced process of local bone resorption and the risk of fracture is greater than in blastic or mixed lesions. According to Mirels´ findings, nearly none of the blastic lesions fractured, but 32% of the mixed lesions and 48% of the lytic lesions did. The erosion in certain locations, such as in the area of femur corticalis and in the humeral area, increases the risk of pathologic fracture because of the dynamic and static load pressure on the long bones.
The intensity of the pain depends on the lesion extent, on the edema of the lesion and its area and on the increased interosseal pressure. The pain getting worse with an increased load indicates an advanced stage of the disease. The subsequent mechanically-induced bone loss may lead to pathologic fracture. The pain exacerbated by movement may predict a pathologic fracture. According to Mirels, while 90% of these lesions measure more than two-thirds of the diameter, the fracture rate increases markedly. The lesions with mild or moderate pain have led to a fracture in only 10% of the cases.
The metastases of the breast cancer, myeloma and cervix uteri represent the lowest risk of pathologic fracture. The metastases of lung cancer represent the highest risk. The risk of fracture increases with age and the stage of overall and local osteoporosis. A frequent site of metastases is perichanter which is a significant load-bearing area leading to a high number of pathologic fractures.
Additionally, pathologic fracture disseminates the tumor cells into circulation causing metastases of primary and secondary tumors. This shortens the survival in primary bone tumors and has a significant impact on patient mortality in cancer metastases to bones. Mirels found that the pathologic fracture indicates the ability of patients to survive less than 6 months with the accuracy of 100% in lung cancer and of 50% in breast cancer.
The Symptoms of Impending or Actual Pathologic Fracture and the Diagnostic Tools
Subjective Symptoms
A large lytic lesion with impending pathologic fracture manifests as intensifying pain. Pain from exposed bone is often produced by weightbearing. Bone erosion induce mechanical deformation and thereby stimulation of receptors in trabecular and cortical layer. Moreover, the bones develop microfractures. A new pathologic fracture is associated with a severe pain. Bone dislocation may lead to serious bleeding. The clinical sign of a fracture include spontaneous pain, hematoma, deformation, crepitus, a pathologic movement and decreased motor function. The hallmark of an impending pathologic fracture is pain intensified with load (function) of the limb.
Establishment of Diagnosis
In the site of a lesion, causing bone resorption, X-ray survey reveals interruption of the bone continuity. (The x-ray can reveal the interruption of bone continuity only when the bone mass is decreased by at least 40-50 %). Fractures may by associated with a dislocation. If the x-ray examination doesn´t report clear finding, it is advisable to perform MR or CT imaging. Technetium scintigraphy of the skeleton helps to reveal other sites of tumor. In multiple myeloma, radioisotope examination MIBI or PET are used to determine the exact location of the tumor. The conventional scintigraphy using technetium pyrophosphate is less efficient in this respect.
Clinical symptoms become obvious only with large lesions at a stage breaching the bone integrity.
Contact Centres:
Clinic of Orthopaedics for Children and Adults, University Hospital, V Úvalu 84, 154 00 Praha 5
Phone: 244 318 808, 8801 (secretary) Eduard Šťastný, M.D.
244 318 803, Josef Mráček, M.D.
E-mail: stastnyed@seznam.cz
Clinic of Orthopaedics, UH Brno Bohunice, Jihlavská 20, 625 00 Brno
Phone: 532 232 765 (amb.), line 2766 (out of work.hours), ass.prof. Richard Chaloupka, M.D.
E-mail: rchaloupka@fnbrno.cz, rgrosman@fnbrno.cz, ortop@fnbrno.cz
Clinic of Orthopaedics, UH u Sv. Anny, Pekařská 53, 656 51 Brno
Phone: 543 181 111 (exchange.), line 2717 (secr.), Head physician René Moster, M.D.
E-mail: rene.moster@fnusa.cz, oldrich.jelinek@fnusa.cz
Conventional X-Ray in two projection images- this methods enable to diagnose the bone involvement by lesions while the bone mass of the skeleton is reduced by 50%,
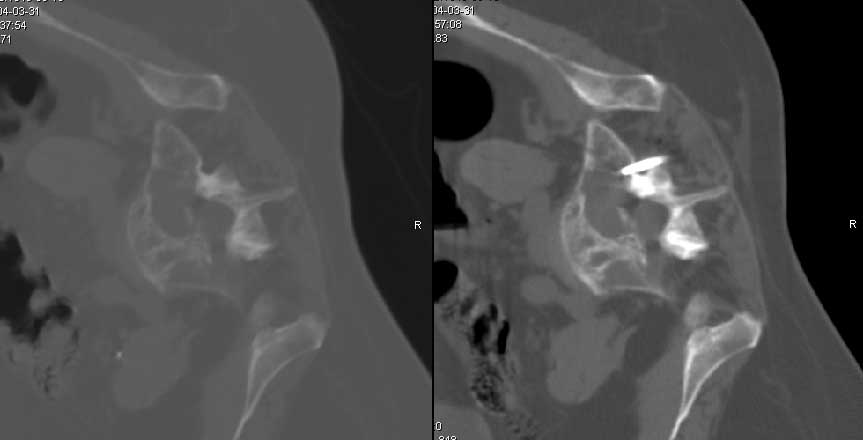
CT - is an important imaging method in axial skeleton involvement, it allows to assess the stability and the discontinuity of posterior elements of the spine
MR - is a "golden standard" allowing to assess the bone marrow involvement by tumor cells, the extent of the extraosseal cancerous bone formation and the infiltration of other tissues.
Biopsy - is a simple percutaneous technique that is minimally invasive. There are virtually no contradictions. Generally, it is necessary to take careful precautions in case of bleeding complications. Lytic lesions that can not be reached by percutaneous route (for example while lesion is in posterior portion of the vertebral body et doesn´t involve any pedicle).
Diagnostic Radiology Capabilities
Indication in patients not eligible for surgical procedure
Methods
RFA - (Radiofrequency ablation) is based on a thermoablation of lytic lesion
The technique is performed by a percutaneous route under local anasthesia. The electrode is positioned in the center of the lesion to coagulate a sphere of tissue. The tumor should be clearly identified at a distance of not less than 0,5 - the safety line - from nerves structures.
Another limitation is the size of the lesion and its infiltration in the subcutis which could represent a relative contraindication to be considered individually.

Cementoplasty - the bone cement is injected in percutaneous route into the lytic lesion. Although, the involvement of a joint or of an intervertebral disc could be a contraindication to this kind of treatment.
Inflammatory lesions or other kinds of inflammatory complications represent an absolute contraindication.
Cementoplasty can be used in combination with prior RFA to achieve the stabilization of the lesion.
Vertebroplasty - the basis of the method lies in percutaneous injection of special bone cement into the vertebral body (cement filling, cement infiltration).
Indications:
Contraindications:
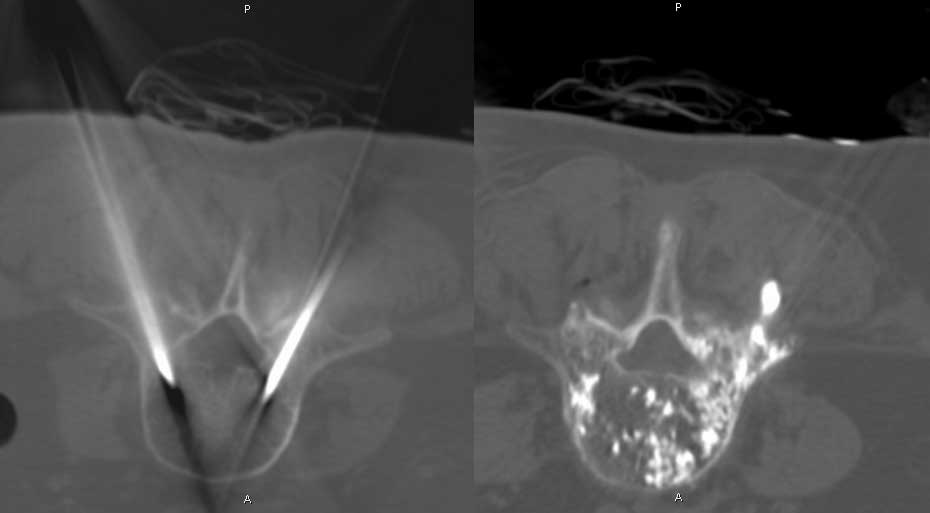
Kyphoplasty - is an offshoot of the vertebroplasty procedure; the difference is that the bone cement is injected into the cavity created with special device in fractured vertebra body or in lesion. This technique permits the vertebral restoration. The compression, resulting from injection into the lesion, creates a pressure valve reducing the risk of blood vessels being blocked by cement leaks. Additionally, the injected cement is not liquid but has the "chewing gum" consistency and its leak is therefore highly unlikely.
The necessity of general anaesthesia represents a disadvantage of this method.
The indications and the contraindications are mostly identical to those for vertebroplasty.
Contact:
MUDr. Jiří Neubauer, UH Brno - Bohunice, Radiology Clinic; Phone: 532 233 549 (CT), 532 233 006 (secretariat)
E-mail - neuba@post.cz, jneubauer@fnb.cz
Radiotherapy
Radiation of lytic lesion in the usual curative dose such as 30 Gy improves outcomes, mainly in terms of local reduction of the cancerous cells and their osteolytic activity. If the mclassant cells are radiosensitive, the reparative process occurs inducing sclerosis of lytic lesion and stabilizing the bone and its normal curvature. It is advisable to perform radiation when Mirels score assesses 7 and less points.
Raditotherapy is a treatment modality in flat bones involvement - ex. ribs, cranial bones, bones of shoulder girdle (the surgical treatment only if strong analgesics can´t achieve pain relief)
According to the Mirels score assessing more than 7 points, the radiation therapy is usually carried out 14 days after the operation when the wound is already healed in case the wound is situated in irradiated field. Otherwise the radiation therapy may follow the operation directly.
The purpose of surgical option is to relieve pain, to restore function in the affected limb or to facilitate care of a patient.
Indication - according to the overall health condition, the survival prognosis and the stage of the disease
ABSOLUTE
RELATIVE
Relative contraindication
First aid
If a pathologic fracture occurs, it is important to immobilize the broken bone like in any other type of fracture (splint, vacuum splint kit, pump, bag Cramer). The plaster cast can´t assure the adhesion of possible fracture fragments and can´t be considered as a definite treatment.
Operative Fracture Stabilization
The orthopedic examination should be undergone as soon as possible after the lytic lesion detection. The use of orthopedic intervention depends on the size, the location, the radiosensitivity (histologic type) of the lesion as well as on the overall survival prognosis. (The orthopedist takes into account the patient´s survival prognosis in treatment strategy consideration to select the optimal surgical procedure).
Survival ranging from 3-6 months: intramedullary nail (palliative intervention) - however, neither the lesion is removed nor the technique promotes fracture healing. In addition, the risk of dissemination of tumor cells in medullar cavity is increased)
Survival over 6 months: resection of the lesion using reconstruction by bone cement and splint to achieve stable osteosynthesis.
Long-term survival: The lesions in tissues surrounding the joint represent an indication for joint replacement (standard tumor arthroplasty) - the lesion is removed and the normal function of the joint are restored within a short period of time (the disadvantage is that the tumor endoprothesis is a costly technique).
Table illustrating the treatment options of impending fractures - prophylactic surgical intervention or radiotherapy?
Procedure in management of large lytic lesions in axial skeleton associated with high risk of pathologic fracture
Aims:
Indications:
Diagnostics:
Treatment:
Occiput - C2 Posterior occipital and cervical stabilization with or without fusion; decompression
Anterior decompression
Combined anterior and posterior stabilization
C3-7 Anterior decompression, vertebral body replacement (bone cement, bone graft and spacers)
Posterior decompression, fusion, instrumentation
Combined interventions
T, L and C spine Posterior interventions - Decompression (poor prognosis)
Decompression and instrumentation (1-year survival rate)
Decompression, fusion, instrumentation (survival rate > 1 year)
Anterior intervention - decompression, vertebral body replacement (bone cement, bone graft and spacers)
Combined interventions - Anterior intervention see above... and posterior fusion, instrumentation, possibly decompression
Centres:
Orthopedic Clinic FH Brno - Phone in amb. 532 232 765, Line 2766 (out of working hours), Associated professor Chaloupka, M.D., Grosman, M.D.
E-mail: rchaloupka@fnbrno.cz, rgrosman@fnbrno.cz, ortop@fnbrno.cz
The Department of Neurological Surgery FH Hradec Králové - Head physician Málek, M.D.
E-mail: malek@fnhk.cz
The Department of Neurological Surgery FH Olomouc - Head physician Vaverka,M.D., Hrabálek M.D.- Phone: 588 441 111
E-mail: vaverkam@tiscali.cz, vaverka.miroslav@seznam.cz
The Department of Neurological Surgery FH Ostrava Poruba - Head physician Paleček, M.D., Phone: 597 375 401
E-mail: tomas.palecek@fnspo.cz
Department of Spondylosurgery Prague FH Motol - Associated professor Štulík - Phone: 602 601 111. Vyskočil, M.D. Phone: 602 604 444, Phone (secretariat): 224 432 580
E-mail: janstulik.spine@seznam.cz
The Department of Neurological Surgery at Hospital Na Homolce - Chrobok, M.D. - 257 273 091, 603 440 105
E-mail: jiri.chrobok@homolka.cz
Orthopedic Clinic ÚVN Praha - Associated professor Klézl Phone: - 602 393 799,
E-mail: klezl.spine@uvn.cz
Orthopedic Clinic IPVZ FN Na Bulovce Prague - Tóth, M.D.
E-mail: toth@fnb.cz
Orthopedic Clinic FH Plzeň Lochotín - Matějka, M.D. - Phone: 377 103 942, 377 103 958
E-mail: matejka@fnplzen.cz
The Department of Neurological Surgery FH Plzeň Lochotín - Head physician Choc,M.D. Runt, M.D.
E-mail: runt@fnplzen.cz
The department of Orthopaedics NsP Ústí n. Labem - Head physician Pilát, M.D.
The Department of Neurological Surgery NsP Ústí n. Labem - Head physician Sameš, M.D.
The Department of Neurological Surgery NsP Liberec - Barsa, M.D.
E-mail: pavel.barsa@nemlib.cz
The Department of Spinal Surgery at Karvinské hornické NsP - Professor Vlach,M.D. Sýkora, M.D.
E-mail: vlach@khn.cz, sykora@khn.cz